Is ISO Certification Worth It? A Cost-Benefit Guide for Businesses
ISO certification is worth it when it helps a business win contracts, meet customer requirements,…

For laboratories, accreditation is the technically correct term.
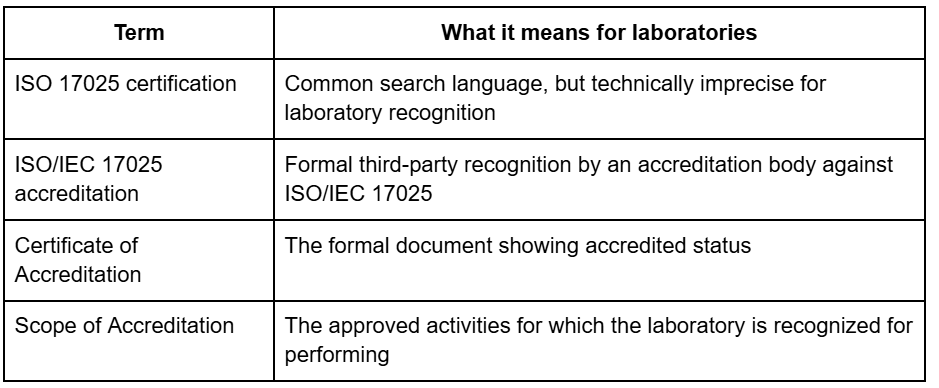
The difference matters because accreditation is not the same thing as a generic certificate. NIST’s NVLAP materials describe laboratory accreditation as an independent third-party assessment of technical competence, based on ISO/IEC 17025, for a specific scope of work.

A laboratory gets accredited by defining its scope, building and operating the system, applying to an accreditation body, completing the assessment, closing any nonconformities, and receiving an accreditation decision. The route is structured, but it is not one-size-fits-all. Scope, technical complexity, and readiness change how much work is involved.
The first real decision is choosing the accreditation body and defining the scope you want to be recognized. Scope is critical because accreditation is granted for specific tests, calibrations, or related activities. ILAC’s signatory search helps laboratories and buyers identify recognized accreditation bodies and, where available, their directories of accredited facilities.
The next step is building the system around how the laboratory actually works. That means documented procedures, technical records, competence controls, equipment controls, traceability logic, result-review practices, and management-system controls that support valid results.
Internal audit and management review are not optional housekeeping tasks. They are key proof points that the laboratory has tested its own system before asking an accreditation body to assess it. A2LA’s accreditation-preparation guidance explicitly includes both before formal assessment.
The external assessment reviews both the documented system and the laboratory’s technical competence in practice. The accreditation body examines the scope, technical work, records, competence, facilities, equipment, and system effectiveness. If nonconformities are raised, the lab must respond with corrective action before the accreditation decision is finalized.
If your scope is clear but your readiness is not, AGS can help before the assessment starts.
That includes scope definition, documentation cleanup, method-readiness review, internal-audit support, and corrective-action planning so the assessment reflects the laboratory’s real competence instead of exposing preventable gaps.
















